
Journal of Clinical Review & Case Reports(JCRC)
ISSN: 2573-9565 | DOI: 10.33140/JCRC
Impact Factor: 1.823



Research Article - (2023) Volume 8, Issue 11
Public Knowledge, Attitude and Practice Behavior towards COVID-19 among Non-Medical Malaysians in Klang Valley
2MAHSA University, Malaysia
3Sungai Boloh Hospital, Malaysia
4Selayang Hospital, Malaysia
5Raja Permaisuri Bainun Hospital, Malaysia
Received Date: Oct 10, 2023 / Accepted Date: Oct 26, 2023 / Published Date: Nov 15, 2023
Abstract
Background: The COVID-19 pandemic was an unavoidable topic in everyone’s life. While the government seeked to reduce the number of cases by spreading information, there was always a question of how much the public actually digests.
Method: To ascertain strategies for better spread of information, this study surveyed 302 participants in the Klang Valley to determine the knowledge, attitude, and practice (KAP) levels of non-medically trained Malaysians towards the COVID-19 pandemic. Due to the movement control order, the questionnaire was cleverly disseminated via an online survey.
Results: The results of the questionnaire showed that there were positive associations between sociodemographic groups such as gender and ethnicity and attitude levels. There was also a significant association between attitude levels and practice levels, in which a high attitude level is greatly associated with high practice level.
Conclusion: This study concluded that knowledge, attitude and practice are having a significant role in prevention of COVID-19.
Keywords
COVID-19, Online survey, Questionnaire, Knowledge, Attitude, Practice, Communication, Malaysia
Introduction
COVID-19 is a viral infection caused by the SARS-CoV-2 (severe acute respiratory syndrome-coronavirus-2). This disease is highly infectious, and its main clinical symptoms may include fever, dry cough, fatigue, myalgia, and dyspnea. The outbreak of COVID-19 is believed to have started in Wuhan City of China back in December 2019. On the 11th of March 2020, the World Health Organization (WHO) declared COVID-19 as a global pandemic with reported cases in most of the countries worldwide (WHO, 2020) [1]. Malaysia and some Southeast Asian countries were among the first countries to report COVID-19 cases outside of China.
The outbreak of COVID-19 in Malaysia was first detected on 25th January 2020, on travelers from China, Hubei arriving in Singapore. It involved three Chinese tourists who had entered Malaysia via Johor. The First 8 cases reported in Malaysia were all imported from China. During the first wave of the COVID-19 outbreak in Malaysia, from Jan 25, 2020 to Feb 26, 2020, there were 22 cases with no deaths reported. The number of cases that were reported remained relatively low and were all imported cases (Malaysia, 2020) [2]. The second wave of the outbreak began on 27 February 2020, and since then the number of people who were affected by COVID-19 rose to more than 1000. To cease the number of new cases, Phase 1 of the Movement Control Order (MCO) was imposed by the Malaysian Government; it commenced on 18th March, 2020 to 31st March 2020. Phase 2 of MCO was implemented and lasted till 14 April 2020. As the number of new cases was increasing, the nation approached the third phase of MCO on 15 April 2020 till 28th April 2020 and has been again extended till 12th May 2020. One of the districts; Klang valley, has been categorized as a red zone of COVID-19 since it has recorded the highest number of confirmed cases (Povera, 2020) [3]. Hence, in this study, we assessed the Public Knowledge, Attitude, and Practice Behavior (KAP) towards COVID-19 among Non-Medical Malaysians in Klang Valley.
In this study, we focused on non-medical personnel, which exclude doctors, nurses, medical assistants, dentists, pharmacists, Chinese traditional medicine practitioners, medical-related students, and any service providers that constitute the practice of medicine or practice of nursing. According to the Ministry of Health Malaysia, there is a ratio of less than 60 registered medical personnel in 10,000 as of 2013 (Pacific, 2014) [4]. We targeted this non-medical audience because medical personnel are deemed to be well-equipped with medical knowledge and tend not to be tainted by unreliable information. Therefore, by assessing the target audience, a more realistic response can be obtained.
The battle against COVID-19 is still ongoing in Malaysia. To guarantee the final success, the public’s adherence to these control measures is essential, which is largely affected by their knowledge, attitudes, practices, and communication behavior towards COVID-19. In this study, we present the findings of an anonymous online questionnaire circulated in Malay and English language to estimate the level of KAP towards COVID-19 among the selected population in Malaysia. The findings of this study are expected to aid in many aspects such as targeting the groups who are less educated in disease transmission, giving insights to the national health policymakers and better planning for awareness campaigns, with all being beneficial for the current pandemic, and also as a good foundation to encounter the next pandemic.
Methodology
2.1 Study design
This study is a cross-sectional study. It is chosen as it is not costly to perform and does not require a lot of time. It also allows different variables to be collected, for example, age, gender, ethnicity, etc. However, it does not help to determine the cause and effect and cannot be used to analyze behavior over a period of time.
2.2 Sample size Since this was an experimental study and prevalence value is not available, the sample size is not calculable by using Kish formula (OpenEpi). Thus, we followed some rules of thumb for determining the sample size by Roscoe. With these rules, together with the number of variables in our study, we derived a sample size of not less than 70.
2.21 Inclusion criteria were
• Malaysian or living in Malaysia
• Able to read in English or Malay
• Willing to participate in the survey
• Non-medical personnel
2.2.2 Exclusion criteria were
• Non-Malaysian or not living in Malaysia
• Illiterate
• Unwilling to participate
• Medical personnel
Convenience sampling was used for data collection. It allowed us to reach the greatest number of people in the shortest amount of time, especially in the MCO period of the COVID-19 pandemic. However, convenience sampling may be vulnerable to selection bias and influence. It also produces a high level of error, skewing the credibility of the study.
An online questionnaire was used to collect data for this study (Figure 1). It was made on a Google Form which could easily be disseminated via a URL link. Responses were collected. It consisted of four parts: Socio-demographics, Knowledge, Attitude, and Practice. The socio-demographic section attains information about the type of people the questionnaire reaches. Knowledge evaluates the level of knowledge by a 3-point Likert scale (True, False, don’t know). Attitude assesses agreeability towards the COVID-19 situation by a 5-point Likert scale (Strongly Agree, Agree, Unsure, Disagree, and Strongly Disagree). Practice also uses a 5-point scale measuring in frequency (Always, Frequently, Sometimes, Seldom, and Never).

Figure 1: Survey Question
2.3 Data analysis
Age variable was categorized into 3 groups (45). There were 6 questions in the knowledge part; the correct answer was given 1 point, while wrong and indecisive answers were given 0 points. The total knowledge score then varied between 0 and 6. Cut off point of ≤4 was evaluated as poor knowledge, and >4 indicated good knowledge.
There were 11 questions in attitude part; 5-point Likert scale responses were reduced to 3 points during analysis, for “Strongly Agree” & “Agree” were given 3 points, Neither Agree/Disagree was given 2 points and Disagree & Strongly Disagree were given 1 point. However, some questions indicated that “Disagree” & “Strongly Disagree” were positive points. The total attitude score then varied from 11 and 33. Cut off point of ≤27 was evaluated as poor attitude, and >27 indicated a good attitude.
There were 6 questions in practice part; “Always” was given 5 points, “Often” was given 4 points, “Sometimes” was given 3 points, “Seldom” was given 2 points, “Never” was given 1 point. The total practice score then varied from 6 and 30. Cut off point of ≤23 was evaluated as poor practice, and >23 indicated good practice.
Data were managed in Microsoft Excel, while statistical analysis was conducted in SPSS Build 1.0.0.1327. Analyses were done and discussed by parts: 1) Socio-demographics, 2) Knowledge, 3) Attitude, and 4) Practice. Frequency, percentage and mean scores were done for univariate descriptive analysis followed by a one-way ANOVA test and Pearson’s Chi-Square test for multivariate cross-tabulation analysis. All the differences of estimated variables were considered statistically significant if p<0.05.
Lastly, thematic analysis was conducted on the open-ended responses at the end of the survey. Out of all responses, only 115 comments are relevant. These comments are further categorized for analysis and some remarkable comments are highlighted. All participants were informed about the aims of this study and gave informed consent. All data were collected in an anonymous database.
Results
A total of 315 participants were involved in this study. 13 nonMalaysian participants were excluded, and it works out to a total of 302 valid respondents. The questionnaire has a 100% completion rate of all the questions.
3.1 Univariate descriptive analysis
3.1.1 Socio-demographics
The mean age of the participants is 30 years old with most of them being 22 years old. 164 (54.3%) of them are 24 or below, 97 (32.1%) are between 25 to 44, and 41 (13.6%) are 45 or above. Of these, 137 (45.5%) were male and 165 (54.6%) were female. The majority of participants were of Chinese and Malay ethnicity, making up 151 (50%) and 129 (42.7%) participants respectively. Other participants were of Indian and Eurasian ethnicity. Most of the participants were either unemployed (47%) or worked in the public sector (34.1%). Finally, most of the participants were university graduates, making up 208 (68.9%) of the sample. The remaining participants finished at primary, secondary, or tertiary education. (Table 1).
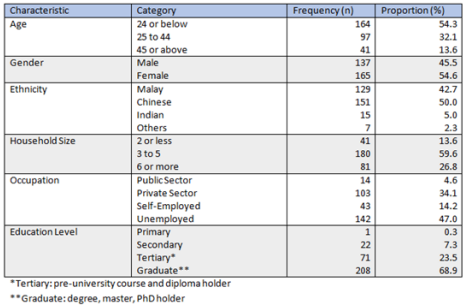
Table 1: Socio-demographics part (n=302)
3.1.2 Knowledge
The majority of respondents correctly answered K1) COVID-19 is a contagious disease-297 (98.3% yes); K5) There is currently no vaccine to prevent-275 (91.1% yes); K6) Social distancing can stop disease spreading-286 (94.7%). Slightly more than half of the respondents correctly answered K3) COVID-19 is a zoonotic disease-170 (56.3% yes) and K4) COVID-19 is a pandemic disease-171 (56.6%). However, only a small portion of respondents correctly answered K2) COVID-19 is caused by bacteria-85 (28.1%). Based on our knowledge level cut off point, there are 143 (47.4%) with good knowledge, and the mean and SD of knowledge score is 4.25±1.083 (0-6) (Table 2).
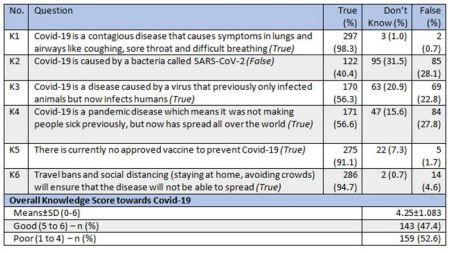
Table 2: Knowledge part (n=302)
3.1.3 Attitude
Majority of respondents agreed on A1) COVID-19 is a deadly disease-220 (72.8%); A2) worried about get infected by COVID-19-278 (92.1%); A3) worried about spreading COVID-19 to others-274 (90.7%); worried about the impact of COVID-19 on work, livelihood and the economy-282 (93.4%); A5) able to by good hygiene and avoid the crowd-297 (98.3%); A6) closure of public areas are unnecessary (disagree)-(66.6%); A7) unwilling to learn about COVID-19 (disagree)-222 (73.5%); A8) obtain most COVID-19 information from official sources-271 (89.7%); A10) willing to share COVID-19 information to friends and family reduce the spread of COVID-19-202 (66.9%); A11) crosscheck information to health agency websites sharing-260 (86.1%). However, only a quarter of respondents agreed on A9) obtain most COVID-19 information from unofficial sources and social media (disagree)-82 (27.2%). Based on our attitude level cut off point, 244 (80.8%) with a good attitud(86.1%). However, only a quarter of respondents agreed on A9) obtain most COVID-19 information from unofficial sources and social media (disagree)-82 (27.2%). Based on our attitude level cut off point, there are 244 (80.8%) with a good attitude, and the mean and SD of attitude score is 29.35±2.512 (11-33) (Table 3).
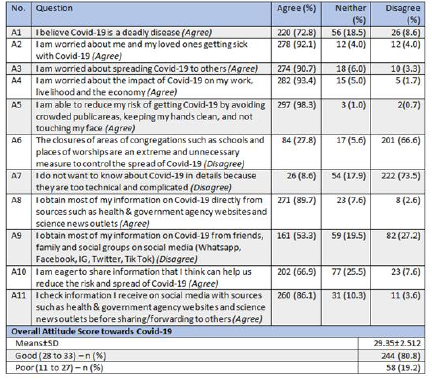
Table 3: Attitude part (n=302).
3.1.4 Practice
In this part, frequencies of Always and Often are combined, indicating good practice towards COVID-19. Majority of respondents have shown good practice in P1) clean hands often with soap and water, or alcohol rubs-276 (91.4%); P2) cover nose and mouth with a bent elbow or a tissue when cough or sneeze-258 (85.5%); P3) stay at home throughout the Movement Control Order (MCO) period except to buy the necessities-289 (95.7%); P4) should wear a mask when going out-274 (90.8%); P5) maintain social distancing when visit a crowded place-296 (98%). However, about two-thirds of the respondents showed good practice in P5) share updated information with friends and family 189 (62.6%). Based on our practice level cut off point, there are 260 (86.1%) with good practice, and the mean and SD of practice score is 26.66±2.999 (6-30) (Table 4).
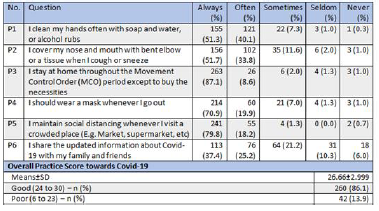
Table 4: Practice part (n=302).
3.3 Multivariate Cross-Tabulation Analysis
3.3.1 Gender and Ethnicity VS Knowledge and Attitude Score
Among the respondents’ ethnicity, the majority are Malay and Chinese, 129 (42.7%), and 151 (50%) respectively. Indian and others are just 22 (7.3%), which is not significant enough for the analysis. Hence, only Malay and Chinese are included under ethnicity in the cross-tabulation analysis. One-way ANOVA and post-hoc multiple comparison analyses found that there is a significant association between gender and attitude (p=0.017), in which females have a higher attitude
score than males. There is also a significant association between ethnicity and attitude (p=0.000), in which Malays have a higher score in attitude than Chinese. This ethnicity-attitude association is extremely strong as the p-value is almost zero. Meanwhile, there is no significant association between gender (p=0.560) and ethnicity (p=0.113) towards the knowledge score (Table 5).
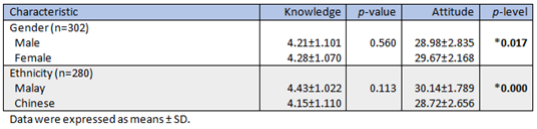
Table 5: Distribution of Knowledge and Attitude Scores among Gender and Ethnicity
3.3.3 Knowledge and Attitude Level VS Practice Level
Pearson Chi-Square analysis found that a significant association between attitude level and practice level (p=0.000), in which a high attitude level is greatly associated with high practice level. There is no significant association between knowledge level and practice level (p=0.104) (Table 6).

Table 6: Person Chi-square Analysis on Knowledge and Attitude towards Practice Level
3.4 Qualitative Analysis
A total of 130 respondents answered the question “What do you think can be done to eradicate a pandemic?” However, after verifying the content of the comments, only 115 comments were used for further analysis.
These comments are then categorized into 1) obey health authority rules and practices; 2) vaccine and cure; 3) knowledge and education, towards the COVID-19 pandemic. This works out a more thematic overview of the respondents’ ideas.
3.4.1 Obey Health Authority Rules and Practices
81 respondents highlighted the need to obey the strict rules implemented by the national health authority, such as travel ban, stay home, and improve personal hygiene and social distancing. Through this, the spreading risk of COVID-19 can be effectively minimized, leading to the possibility of eradication of the pandemic.
“I think everyone should just comply with whatever our government has and going to decide as they know about this pandemic better. RMO has been working well so far so I guess we should just keep it going until KKM found a better measure to stop this pandemic.” (Respondent 46, 24th April 2020).
“Focus on improving personal health while following the strict orders of the government and health professionals to the best of my abilities.” (Respondent 72, 24th April 2020).
3.5 Vaccine and Cure
21 respondents suggested that the introduction of vaccines or cures were of utmost importance to stop a pandemic. They are in hope that global health experts can come up with vaccines and a cure for COVID-19 as early as possible.
“There is no easy solution I guess. The months ahead will involve a fragile balancing act between the interests of public health, society, and the economy, with governments more reliant on each other than ever before. While half the battle will be in developing the tools to treat the virus-like a vaccine, antiviral therapies, or some diagnostic testing bah. Then for the other half, I think will be manufacturing enough doses bah as distributing these fairly and equitably, and ensuring they reach individuals across the world. ” (Respondent 49, 24th April 2020).
“Furthering research on injection of disinfectants to cure the virus. Looking into essential oils and homeopathic alternatives. ” (Respondent 210, 25th April 2020).
3.6 Knowledge and Education
11 respondents highlighted that knowledge and education are necessary to prevent and control a pandemic. Knowledge and education regarding COVID-19 and any disease pandemic have to be circulated effectively to everyone with the aid of global and national health authorities, both before and after the pandemic outbreak.
“Clear knowledge and swift action by Govt of the country is necessary to prevent a mass outbreak. Also, having an efficient centralized reporting procedure is crucial for data gathering. ” (Respondent 217, 26th April 2020). “To always be aware of the pandemic before it becomes viral and takes all the necessary steps to prevent it. The earlier we do these the faster we can eradicate the pandemic. ” (Respondent 238, 27th April 2020).
Last but not least, a very comprehensive and insightful comment obtained from the survey are shown below:
“Countries should treat the COVID-19 pandemic as an actual war on the scale of the World Wars (albeit invisible one) instead of just a temporary annoyance. Ignoring the problem won’t make the problem go away. Drastic problems require drastic solutions.
It is during times of crisis/wars where innovation occurs. Countries should focus on unifying their efforts in combating COVID-19 through global localization where efforts are made at all levels scaling from the international sphere to grassroots. This requires research to be free and accessible to the public, governments to adapt and collaborate, and communities to work together. It takes one super spreader to infect thousands, thus everyone must be united in combating COVID-19. Thus this requires all segments of society (including indigenous communities, B40, migrants, ‘illegal’ documented workers, refugees, etc) to be unified. The virus doesn’t care if you’re rich or poor, if you get it, you get it.
Education & adaptation should be prioritized. The west wasted too much time arguing about whether PPE/masks are useful. What’s been done has been done so all efforts should be focused on the present & future. Geopolitics (such as countries blaming China) can come later as blame won’t do much at the present moment though federal politics is another issue (e.g. USA, Brazil, etc with leaders who prioritize reopening the economy over public health). Leaders should listen to scientists/doctors/ public health officials and regard the pandemic as a public health war instead of only focusing on the economy. There won’t be an economy if there’s no civilization left.
A change in mindset is crucial and good leadership is a must. Leaders must be proactive and not reactive - it is better to take drastic actions and be regarded as ‘paranoid’ rather than regret, panic, and react later on. We need to think 10, 20, 100 steps ahead even though it is hard to navigate such unprecedented situations. We are living through a historical event that will be marked down on future history textbooks.” (Respondent 246, 27th April 2020).
Discussion
The rising number of COVID-19 cases have crafted frustration and apprehension in the nation as there were still number of citizens who failed to adapt and adhere to the country’s Movement Control Order. In our view, knowledge, practice and attitude of any group of people towards whichever form of outbreak depicts the outcome in flattening the COVID-19 curve. Hence, in this study we were assessing the Public Knowledge, Attitude and Practice Behavior towards COVID-19 among NonMedical Malaysians in Klang Valley.
The findings in our study showed that about half of the respondents (47.4%) are equipped with good knowledge score towards COVID-19. 98.3% of the respondents are well aware of the symptoms of COVID-19 and have good knowledge that it is contagious.
97% of the respondents were recorded to have good knowledge in Movement Control Order which is much required in breaking the chain of COVID-19 transmission in Malaysia; as they are very much aware of social distancing, crowd avoidance and travel bans. Ever since the emergence of this outbreak, Malaysia Ministry of Health had joined hand together with Malaysia Communication and Multimedia Commission (MCMC) to disseminate various information on COVID-19 to the public. As health science related communication is primarily seen as endeavor in transmitting new information through formal or informal approach such as through media (Kappel and Holmen, 2019) [5]. On Exception, only 28.1% were well aware of that COVID-19 is due to a virus, not bacteria origin. These results are in line with the findings from Dauda et al. [6]. Another important finding from our study was obtained by assessing the public’s attitude towards COVID-19, 80.8% of the respondents displayed good attitude. Overall, a vast number of respondents have positive attitude towards COVID-19 mainly can be associated with good knowledge too.
However, there were 84 respondents which comprises of 27% of the total respondents, feels that the closure of schools and worship places are rather extreme and unnecessary act. This number depicts that there are still 27% of the total respondents are somewhat lacking in their knowledge to understand the implication of unrestricted movement during the outbreak. Poor knowledge and awareness towards COVID-19 could be the reason for poor attitude as well. This can be supported by a study done in Korea on 2015 (Ko et al., 2015) [7].
In our study analyses, we found that there is a significant association between gender and attitude (p=0.017), in which female has higher attitude score than male. Our results are comparable to the findings of similar study on COVID-19 (Moorthy et al., 2020) [8].
Based on our practice level cut off point, there are 260 (86.1%) displayed with good practice in which 87.1% of the respondent are totally in adherence of MCO rules; they practice ‘stay at home’ and do not go out till its necessity arrive. 70.9% of the respondents implementing good practices by wearing mask whenever they go out, and this can be strongly related to good attitude as according to our analysis, high attitude level is greatly associated to high practice level. Only 1.0% of the respondents failed to adhere good practice towards COVID-19, mainly in obeying MCO, usage of mask and failure in covering nose/ mouth while sneezing and coughing. Hence it is comprehended that majority of our respondents took precautions to avoid COVID-19 contamination.
Meanwhile, the findings of the study have statistically proven most of our research hypotheses. While most of the null hypotheses are rejected, some of them could not be rejected due to lack of significance. (1) There is a high level of knowledge towards COVID-19 in non-medical Malaysians (NMM); (2) There is a positive association between knowledge and practice towards COVID-19 in NMM. (3) There is an association between socio-demographics and the level of attitude towards COVID-19 in NMM.
The particular aspect of the COVID-19 pandemic that interested researchers is the difference between the levels of knowledge, attitude, practice (KAP) and the socio-demographic groups of the population. The information is essential as any association and correlation between them could be of high value and provide insight to the local health authority, allowing them to act accordingly and effectively. Fortunately, most studies have agreed on this topic to a great extent. However, few studies have shown contraindicating findings.
Different countries have different healthcare systems, potentially causing a major impact on their population’s KAP towards COVID-19 pandemic. Several studies have shown that countries like China, USA, India, Malaysia, Vietnam, and Peru have a good overall KAP level towards COVID-19. In contrast, a study in Thailand showed that the overall KAP level was poor, perhaps due to the study participants’ extreme living conditions at the Thai border (Srichan et al., 2020) [9]. While knowledge and attitude levels are good in most countries, practice and behavior are otherwise less satisfactory (Giao et al., 2020) [10].
Association between the socio-demographic groups and KAP levels towards COVID-19 among the population is also essential to determine which particular group is at higher risk. The most prominent associations are between gender, education level, and economical status. Few studies found that participants who are female, have a higher educational level, and economical status have a positive association with overall KAP level (Zhong et al., 2020) [11].
Meanwhile, the association, and perhaps the casual relationship, between knowledge, attitude, and practice behavior can give us an idea on which aspect is more important than the others. For instance, knowledge and information tend to influence people’s behavior (Khayriyyah and Chang Da, 2020) [12]. Most studies have shown an apparent positive correlation between knowledge towards attitude and practice behavior (Latiff et al., 2012) [13]. However, one study conducted in Malaysia back in 2018, showed a negative correlation, which is the opposite. The participants of this study are Islamic pastors and teachers. While having good knowledge of respiratory tract infections, they have a very poor attitude and practice behavior towards it (Dauda Goni et al., 2019) [6]. This finding, however, does not represent the entire Malaysian population.
The KAP level has always been increasing with the enhancement of healthcare technology, the aid of local health authority, and also the communication improvements achieved by the Internet and social media platforms. In Malaysia, studies have shown a significant increase in overall KAP level towards respiratory illness pandemics. Malaysian showed moderate to poor KAP level towards H1N1 according to few studies back in 2012 (Latiff et al., 2012) [13], whereas good KAP level is found towards COVID-19 (Khayriyyah and Chang Da, 2020) [12]. This is a good trend that should continue for Malaysians to solve the current COVID-19 pandemic and also prepare for the next one. On the other hand, other studies also showed interesting findings. Medical students are found to have no difference from nonmedical students on the overall KAP level towards COVID-19 by a study conducted in Jordan (Alzoubi et al., 2020) [14]. A study in Vietnam also showed that people are more reliant on social media than the ministry of health for knowledge towards COVID-19 (Giao et al., 2020) [10].
Despite the wide range of information, more studies need to be conducted to obtain a more accurate KAP level of the population towards the COVID-19 pandemic. After this, a comprehensive association among different socio-demographic groups and KAP variables can be derived. The findings, then, can be utilized by the local health authority to wisely allocate the limited resources and implement effective general health policy, targeting the vulnerable groups among the population.
Limitations
While there are strengths to this study, there are many areas that can be improved. One of the biggest limitations is the survey questions. Some of them are badly phrased and can be interpreted wrongly. A solution to this is a proper review of the questions by control groups before sending it out for data collection. The distribution of the questionnaire was also limited due to the COVID-19 lockdown. Optimally, we would also approach the public in person, also allowing us to get a larger sample size. The KAP scoring was also flawed due to the cutoff points. Because the score was made-up by the study team, there was no significant rationale behind the scoring system, possibly skewing the data. Another cause of data skewing is the repetition of questionnaire answers. Some participants might have accidentally sent in two responses instead of one, causing the sample size to be more than it is.
Conclusion
From this study, it can be derived that the general population of Malaysia have modest knowledge, good attitude and practice towards COVID-19. The latter two reflect the effect of the MOH’s efforts in guiding the public to prevent further spread of the disease, whereas the former, may indicate the need for better strategies to bring awareness and education to them. The findings of this study may prove as the foundation for planning awareness campaigns among the public and helpful in directing the efforts and plans of the health authorities of the country for better containment of COVID-19.
Recommendations
There are a few things that can be done by the health authorities to improve the overall knowledge, attitude, and practices towards COVID-19 in Malaysia. For example, the information about COVID-19 can be shown in different languages so everyone can understand it better. Next, the health authorities can educate Malaysians regarding the knowledge about COVID-19 (e.g., the causative agent, meaning of pandemic, etc.) in a form of animation as it can be more easily understood by Malaysians from different age groups. Furthermore, the health authorities can explain more about the rationale behind each action they have taken (e.g., MCO), so the people will be more willingly to comply and don’t break the rules as easily after understanding the rationale. With all these efforts, I believe we can achieve a higher level of knowledge, attitude, and practice towards COVID-19 in Malaysia.
Funding Sources
There is no funding.
Conflict of Interest Statement
The authors have no conflict of interest to declare.
Acknowledgement
The authors would like to thank all the questionnaires providers, MAHSA University, and Supervisor Dr Than Tun Aung for critical input to the manuscript.
References
1. WHO (2020). COVID-19 situation reports [Online]. Available: https://www.who.int/emergencies/diseases/ novel-coronavirus-2019/situation-reports [Accessed 2020].
2. Malaysia, D.O.S. (2020). CoVID-19 Current Situation in Malaysia. Malaysia.
3. Povera, A. (2020). 4 locations in KL identified as Covid-19 red zones New Straits Times.
4. Pacific, W.R.O.F.T.W. (2014). Human resources for health country profiles: Malaysia. Manila: WHO Regional Office for the Western Pacific.
5. Kappel, K,. & Holmen, S.J. (2019). Why Science Communication, and Does It Work? A Taxonomy of Science Communication Aims and a Survey of the Empirical Evidence. Frontiers in Communication, 4.
6. Dauda Goni, M., Hasan, H., Naing, N.N., Wan Arfah, N., Zeiny Deris, et al. (2019). Assessment of Knowledge, Attitude and Practice towards Prevention of Respiratory Tract Infections among Hajj and Umrah Pilgrims from Malaysia in 2018. Int J Environment Res Public Health, 16, 4569.
7. K0, H.S., Jo, Y., Kim, Y., Park, Y.G., Moon, H., et al. (2015). Knowledge, attitudes, and acceptability about influenza vaccination in Korean women of childbearing age. Obstetrics & Gynecology Science, 58, 81-9.
8. Moorthy, V., Restrepo, A., Peziosi, M.P., & Swaminathan, S. (2020). Data sharing for novel coronavirus (COVID-19). Bulletin of the World Health Organization, 98(3), 150.
9. Srichan, P., Apiechkul, T., Tamornark, R., Yeemard, F., Khunthasn, S., et al. (2020). Knowledge, Attitude and Preparedness to Respond to the 2019 Novel Coronavirus (COVID-19) Among the Bordered Population of Northern Thailand in the Early Period of the Outbreak: A CrossSectional Study. WHO South East Asia J Public Health, 9(2), 118-125
10. Giao, H., Thi, N., Thi Ngoc Han, N., Khanh, T., Ngan, V., et al. (2020). Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pacific J Tropical Medicine, 2020.
11. Zhong, B.L., Luo, W., Li, H.M., Zhang, Q.Q., Liu, XG., et al. (2020). Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online crosssectional survey. Int J Biological Sciences, 16, 1745-1752.
12. Khayriyyah, M.H., & Chang, DA. (2020). Public knowledge, perception and communication behavior surrounding COVID-19 in Malaysia. 2020.
13. Latiff, L.A., Parhizkar, S., Zainuddin, H., Chun, G.M., Rahiman, M.A.A., et al. (2012). Pandemic influenza A (H1N1) and its prevention: a cross sectional study on patients’ knowledge, attitude and practice among patients attending primary health care clinic in Kuala Lumpur, Malaysia. Global Journal Of Health Science, 4, 95-102.
14. Alzoubi, H., Alnawaiseh, N., Al-mnayyis, A.A., Lubad, M., Aqel, A., et al. (2020) COVID-19 -Knowledge, Attitude and Practice among Medical and Non-Medical University Students in Jordan. J Pure and Applied Microbiology, 14, 17-24.
Copyright: © 2025 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.