
Journal of Clinical Review & Case Reports(JCRC)
ISSN: 2573-9565 | DOI: 10.33140/JCRC
Impact Factor: 1.823



Case Report - (2023) Volume 8, Issue 8
Chondrosarcoma of Pubic Bone in Pregnancy: A Case Report
Received Date: Jun 09, 2023 / Accepted Date: Jun 29, 2023 / Published Date: Aug 31, 2023
Abstract
Cancers are rare during pregnancy and diagnosed in about one per 1000 deliveries. Bone cancers account for only 0.2% of all malignancies. Cancers of the pelvic bones during pregnancy constitute specific challenges to both orthopedic oncologists and obstetricians. Thirty one year old primigravida at 23 week gestation presented with 15 cm chondrosarcoma on the left pubic bone. She was delivered by elective caesarean section at 37 week gestation. Surgical resection of the malignant tumor was performed postnatally.
Keywords
Oncologists, Obstetricians, Pelvic bones, Pregnancy, Chondrosarcoma
Introduction
Cancer diagnosis during pregnancy is a rare coexistence in a ratio of one case per 1000 deliveries. However, there is an increasing trend due to delaying pregnancy in western societies into the later reproductive years [1].
The most common gestational cancers are those appearing during the reproductive period of a woman. Breast cancer and cervical cancers are the most frequently diagnosed malignancies followed by hematological tumors and melanoma [2].
Malignant bone tumors are rare, accounting for only 0.2% of all malignancies. Among them the most frequent are osteosarcoma, Ewing’s sarcoma and chondrosarcoma. They are rarely diagnosed during pregnancy. In a recent review 38 cases of malignant bone tumors during pregnancy were reported over a 50 years period (1963-2014). Only 10 cases of these were gestational chondrosarcomas [2].
Chondrosarcoma is more commonly diagnosed over the age of 40. Most frequently it affects the pelvis, axial skeleton and proximal limbs. Histologic grading is important ranging from grade 1 to 3. The primary modality of therapy is surgery. Fiveyear survival is more than 90% and 25% for grade 1 and 3, respectively.
Diagnostic and staging workup should be very carefully performed due to maternal and fetal radiation exposure. Recommendation of imaging studies should always follow the established guidelines.
Case Report
A 29 years old lady from Philippine, presented to a local hospital in March 2019 with pelvic pain and urinary frequency. MRI showed a large pelvic mass. Biopsy was consistent with osteochondroma. She underwent partial resection of the mass in OCT 2019. The post-operative histopathology showed: Secondary chondrosarcoma, Grade 1, arising in osteochondroma. There was no evidence of higher grade chondrosarcoma (Grade 2,3) or dedifferentiation.
After partial tumor resection, the patient had follow up imaging done in 2020, including CT angiography which showed the residual lesion measuring 12.2x9x9.5 cm (SIxAPxTR). There was local extension into the left rectus abdominous muscle which shows a large hypodense component measuring 4.5x2.5cm. The inferior component of the lesion along the femoral canal measures 7.2x6.1x5.4cm.
MRI pelvis showed evidence of heterogeneous mixed intensity lesion in the left side of pelvis extending laterally and inferiorly to reach the subcutaneous plane in the left inguinal region. The residual lesion measures approximately 15.4x10.6x11.7cm in size (Figure 1,2).
During the investigation the patient found herself pregnant and that delayed further treatment.
In March 2021 the patient was referred to orthopedic oncology team in our hospital. She was then 31 years old, primigravida and she was 23 weeks pregnant, with left pelvic chondrosarcoma. Multidisciplinary team meeting was made with the obstetricians and orthopedic doctors to plan management and delivery date for the patient. It was decided that the mode of delivery will be by an elective cesarean section at 37 weeks of gestation.
The patient was on prophylactic dose of low molecular weight heparin (LMWH) through her antenatal period. She was diagnosed with left leg deep vein thrombosis (DVT) at 28 weeks, and the LMWH was switched to therapeutic dose. An ultrasound scan was done at 36 weeks showed normal growing fetus, normal placental localization, and a transverse fetal lie.
Betamethasone 2 doses was given for fetal lung maturity, LMWH was stopped for 24 hours before the surgery.
Abdominal examination showed Large (15 cm) solid tumor arising from the pubic bone extending to 5 cm below the umbilicus, markedly tender on palpation, the tumor was pushing the gravid uterus and the uterine contents upwardCesarean delivery was performed in June 2021 at 37 weeks gestation through a high longitudinal midline incision at the level of the umbilicus. There was a large 15 cm solid mass arising from the pubic bone extending upward toward the umbilicus preventing direct access to the lower uterine segment and bladder, therefore a high longitudinal incision was made on the upper uterine body. A healthy female baby was delivered by breech extraction. The uterus was closed in two layers.
The patient had uneventful post-operative recovery and she was discharged on day 6 post-operatively.
The patient continued follow up under the orthopaedic oncology team postnatally. Radical resection of G1 chondrosarcoma of the left pubic bone was performed in September 2021. The patient made good postoperative recovery and discharged home 10 days later. The patient then has regular follow up with the orthopedic oncology team.
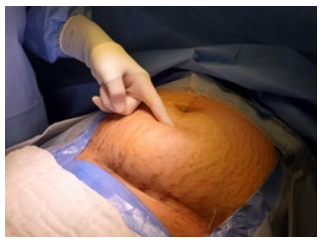
Figure 1: Chondrosacoma of pubic bone reaching to 5 cm below the umbilicus

Figure 2: Chondrosacoma of pubic bone blocking the uterine lower segment intraoperatively
Discussion
Considerable delay in the surgical excision of this malignant tumor (2019-2021) was caused by referral and insurance issues and by the pregnancy.
In our case the malignant tumor of the bone was diagnosed prior to the pregnancy. Therefore, no biopsy and no extensive imaging for the tumor was needed during the pregnancy.
Grade 1 chondrosarcoma has a favorable prognosis. This allowed the pregnancy to continue to term and a planned treatment resection of the tumor postnatally. Removing this large tumor of the pubic bone during pregnancy was technically not possible.
The location of the tumor in the pelvis prevented vaginal birth, and the position of the tumor in front of the uterus posed technical challenge during Cesarean section. The large pubic tumor in our case prevented access to the lower uterine segment. So classical cesarean section had to be performed, and the suitable skin incision in this situation was longitudinal above and below the umbilicus.
References
1. Pentheroudakis, G., & Pavlidis, N. (2006). Cancer and pregnancy: poena magna, not anymore. European journal of cancer (Oxford, England) 42(2), 126-140.
2. Zarkavelis, G., Petrakis, D., Fotopoulos, G., Mitrou, S., & Pavlidis, N. (2016). Bone and soft tissue sarcomas during pregnancy: A narrative review of the literature. Journal of advanced research, 7(4), 581-587.
Copyright: © 2025 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.