
Journal of Clinical Review & Case Reports(JCRC)
ISSN: 2573-9565 | DOI: 10.33140/JCRC
Impact Factor: 1.823



Case Report - (2023) Volume 8, Issue 7
Cecal Volvulus: Case Series Study
Received Date: Jul 12, 2023 / Accepted Date: Jul 20, 2023 / Published Date: Jul 30, 2023
Abstract
Cecal volvus (CV) is considered to be a rare cause of intestinal obstruction, it occurs when the ascending colon and the terminal ileum are twisted around their mesenteric pedicle, resulting in a closed-loop obstruction, CV counts about 1- 1,5% of all intestinal obstructions [1]. Its clinical features are those of the other forms of intestinal obstruction which make the imaging screening crucial for a prompt diagnosis in order to reduce the high mortality rate due to the intestinal necrosis or perforation [2].
We report a case series of 6 patients who were admitted mostly for abdominal pain and vomiting and for whom radiological investigations confirmed a cecal volvulus which was successfully managed by the surgical teams, no recurrence has been noted so far.
Keywords
Intestinal obstruction, surgery, Cecal volvulus, Abdominal surgery, Intestinal necrosis, Neuroleptic drugs, Laparoscopic examination, Paralytic ileus
Abbreviations
CV: Cecal Volvulus; CT: Computerized Tomography
Introduction
Cecal volvulus is the second most common type of colonic volvulus after sigmoid volvulus [3] accounting for approximately 10% of all intestinal volvuluses.
Cecal volvulus occurs in case of inadequate right colon fixation or congenital abnormalities in which the right colon does not properly fuse with the lateral peritoneum [4].
Based on reports from necropsy reviews, sufficient cecal mobility for volvulus and bascule formation is found in 11% and 25% of adults, respectively. In addition of cecal fixation abnormalities, other risk factors include: high fibre diet, chronic constipation, abdominal masses, late-term pregnancy, previous abdominal surgery, prolonged immobility, paralytic ileus, neuroleptic drugs and colonoscopy [4]. If not treated on time, CV can lead to drastic complication due to obstruction and twisted mesenteric vessels leading to intestinal necrosis.
In terms of diagnosis, the clinical and biological findings are unspecific which makes the radiological imaging crucial for a positive diagnosis.
Case Studies
2.1 Case 1
A 65-year-old female was admitted for an abdominal pain with nausea and vomiting of three days duration, she has a history of hypertension and diabetes. A physical examination on admission showed a vastly distended abdomen which was non-tender, Hemodynamic and respiratory values were normal: 122/76 mmHg of blood pressure, and a 95 hbpm. Initial laboratory investigations were unremarkable.
An Initial abdominal plain film showed gross colonic distension with likely large bowel obstruction, then a CT scan was perfomed which confirmed a cecal volvulus (Figure 1).
The patient underwent an urgent surgery. The laparoscopic examination showed a mobile caecum caused by the elongated ascending colon. An ileocecal resection with mechanical latero-lateral ileocecal anastomosis was perfomed associated to cecopexy.
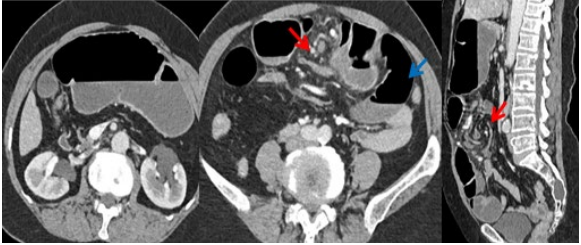
Figure 1: The markedly dilated cecum is located in the upper abdominal quadrant (White arrow). It shows air-fluid level, thickened walls & stranding densities in the surrounding mesentery. There is twisting of the medial side of mesenteric fat & vessels resulting to a tornado-like appearance “whirl sign” (Red arrow). Dilated fluid-filled small bowel loops are seen (blue arrow). The rest of the colon are collapsed. Reference: Radiology department CHU HASSAN II, FEZ, Morocco.
2.2 Case 2 A 33-year-old man who consulted for an abdominal distention, he estimated that his bowels had not opened for more than 2 days. He has a history of smoking and chronic constipation.
Physical examination showed a markedly distended abdomen that was soft and mildly tender and his vital signs showed no significant abnormality. Initial abdominal plain film showed a grossly distended colon with large bowel obstruction. Computed Tomography (Figure 2) showed a markedly distended caecum.
These findings were suggestive of a CV.
The decision was to admit the patient to the operating room. The laparoscopic examination showed a cecal volvulus complicated by perforation. An ileocecal resection with double stoma was performed.
The patient had good postoperative recovery and was discharged from the hospital on the fourth day following the operation. A restoration of intestinal continuity was made later.
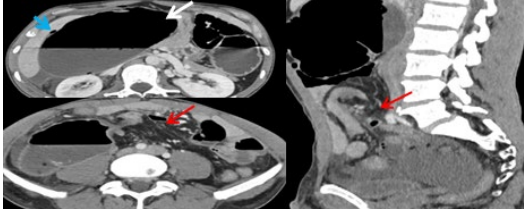
Figure 2: The markedly dilated cecum is located in the upper abdominal quadrant (White arrow). There is twisting of the right side of mesenteric fat & vessels resulting to a tornado-like appearance “whirl sign” (Red arrow). We notice the pelvic position of transverse colon, It is associated with pneumoperitoneum and an intraperitoneal effusion (blue arrow). Reference: Radiology department CHU HASSAN II, FEZ, Morocco.
2.3 Case 3
A 5-year-old girl was admitted because of severe abdominal pain, nausea, and vomiting since the previous 2 days. There was no history of abdominal procedures, His pulse rate was 100 beats/min, temperature was 37°C, and blood pressure was 110/70 mmHg. Physical examination revealed severe abdominal distension and tenderness. Computed Tomography (Figure 3) showed a cecal volvulus.
The patient was admitted to the operating room. The laparoscopic examination showed a cecal volvulus. A devolvulation was perfomed associated to cecopexy.
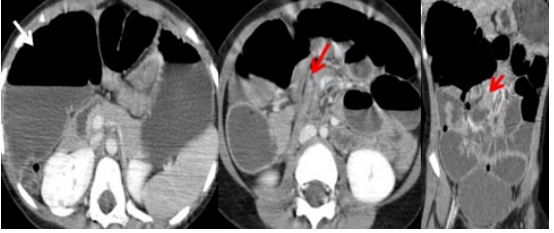
Figure 3: The markedly dilated cecum is located in the upper abdominal quadrant (White arrow). There is twisting of the right side of mesenteric fat & vessels resulting to a tornado-like appearance “whirl sign” (Red arrow). Reference: Radiology department CHU HASSAN II, FEZ, Morocco.
2.4 Case 4
A 17-year-old male was admitted to the emergency departement for a 3-day history of colicky abdominal pain, he was afebrile and hemodynamically stable. On examination, his vital signs were within normal levels. The abdomen was distended, with muscle guarding and rigidity throughout. Peristaltic sounds were hyperaudible. Erect radiograph of the abdomen showed multiple air-fluid levels. Computed Tomography (Figure 4) showed a cecal volvulus.
Due to the spontaneous resolution of symptoms, the patient was referred for colonoscopy and then lost to follow-up.
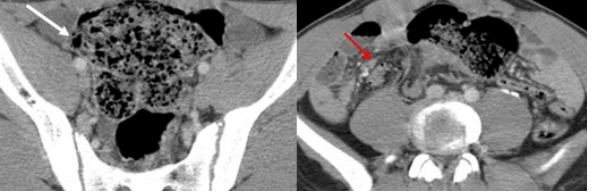
Figure 4: The dilated cecum is located in the pelvis (White arrow). It shows air-fluid level and stranding densities in the surrounding mesentery. There is twisting of the right side of mesenteric fat & vessels resulting to a tornado-like appearance “whirl sign” (red arrow). Reference: Radiology department CHU HASSAN II, FEZ, Morocco.
2.5 Case 5
A 53-year-old male was admitted to the emergency departement for a 4-day history of colicky abdominal pain. On examination, his vital signs were within normal levels. The abdomen was distended, with muscle guarding and rigidity throughout. Initial abdominal plain film showed a grossly distended colon with large bowel obstruction. Computed Tomography (Figure 5) showed a cecal volvulus caused by an incomplete intestinal malrotation.
The patient underwent an urgent surgery. The laparoscopic examination showed a mobile caecum caused by an intestinal malrotation with elongated ascending colon. A detorsion was perfomed associated to cecopexy.
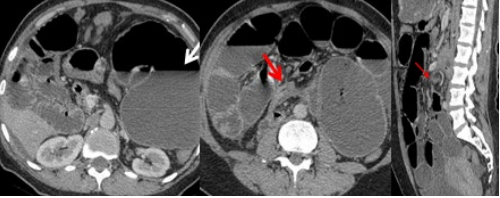
Figure 5: The markedly dilated cecum is located in the left upper abdominal quadrant (white arrow). Its transverse diameter is more than 10 cm in its widest portion. It shows air-fluid level and stranding densities in the surrounding mesentery. There is twisting of the right side of mesenteric fat & vessels resulting to a tornado-like appearance “whirl sign” (red arrow). Dilated fluid-filled small bowel loops are seen. The rest of the colon are collapsed. Reference: Radiology department CHU HASSAN II, FEZ, Morocco
2.6 Case 6
A 24-year-old male with history of appendectomy (Notion of left appendix) was admitted to the emergency departement for severe abdominal pain, nausea, and vomiting since the previous 4 days. On examination, the abdomen was distended, with muscle guarding and rigidity throughout. Initial abdominal plain film showed a grossly distended colon with large bowel obstruction. Computed Tomography (Figure 6 and Table 1) showed a cecal volvulus caused by an intestinal malrotation. The patient underwent an urgent surgery. The laparoscopic examination showed a cecal volvulus caused by an intestinal malrotation with adhesive bands. A detorsion was perfomed associated to excision of bands and cecopexy.
| Case | Symptoms | Imaging | Complications | Laparoscopic Examination | Treatment | Outcome |
|---|---|---|---|---|---|---|
| 1 | Abdominal pain, nausea and vomiting | Whirl sign, collapsed colon | None | Mobile cecum caused by the elongated mesocolon | Ileocecal resection with mechanical latero-lateral ileocolonic anastomosis with cecopexy | Favorable |
| 2 | Abdominal distension, pain, vomiting with absolute constipation | Whirl sign, pelvic position of transverse colon | Proximal necrosis and perforation | Cecal volvulus confirmed laparoscopically | Ileocecal resection with mechanical anastomosis and cecopexy | Restoration of intestinal continuity |
| 3 | Abdominal pain, distension, and vomiting | Whirl sign, abnormal position of cecum and the appendix in the upper abdominal quadrant | A greatly distally dilated intestine with perforation of a loop | Devolvulation and evacuation of intestinal contents | Devolvulation and evacuation of intestinal contents | Favorable |
| 4 | Colicky abdominal pain, the patient was febrile | The dilated cecum is noted in the pelvis | None | No laparoscopic procedure | Due to the patientâ??s refusal to perform surgery, medical follow-up was preferred | Lost to follow-up |
| 5 | Colicky abdominal pain | Whirl sign, abnormal position of the cecum, incomplete intestinal obstruction | None | Mobile cecum and volvulus detected during laparoscopic surgery | Adhesiolysis and anterior cecopexy with intraperitoneal fixation | Favorable |
| 6 | Severe abdominal pain, nausea, vomiting | Whirl sign, incomplete pain, and abnormal orientation of the SMA & SMV | None | Cecal volvulus confirmed and treated laparoscopically with intestinal adhesion and adhesive bands | Detorsion and cecopexy with adhesion band release and cecopexy | Favorable |
Table 1: Summary table of patients
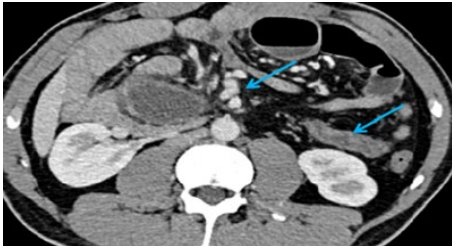
Figure 6: The markedly dilated cecum is located in the right abdominal quadrant (White arrow). Its transverse diameter is more than 10 cm in its widest portion. There is twisting of the middle of mesenteric fat & vessels resulting to a tornado-like appearance “whirl sign” (red arrow). The position of the colon in the left flank associated with an abnormal orientation of the SMA & SMV suggest an intestinal malrotation (blue arrow). Reference: Radiology department CHU HASSAN II, FEZ, Morocco.
Discussion
Though several factors predispose to cecal volvulus, it is believed that the major predisposing factors are the presence of a mobile caecum and a fixed point of rotation [6]. According to some studies a mobile caecum is an anatomical variant, present in 25% of the general population [6].
This mobility is caused by deficient colonic fixation to the peritoneum or colon elongation resulting from over-rotation during embryologic development [7].
The symptoms and laboratory abnormalities of cecal volvulus remain unspecific and are determined by the duration and the severity of the intestinal obstruction, in the acute obstruction form the patient may suffer from a cramping abdominal pain associated to vomit, abdominal distension and trouble passing gas, whilst in the stage of bowel necrosis the patients have generally a toxic appearance with peritonitis signs.
In terms of diagnosis, Abdominal radiography may allow a diagnosis if three typical signs are present: Caecum dilatation, a single air-fluid level in the right lower quadrant, and absence of gas in the colon. However, up to 30% of patients do not show these radiographic features [8]. Computerized tomography is considered to be the imaging technique of choice, allowing not only confirmation of the diagnosis, but also ruling out other causes of acute obstruction. Coffee bean, bride beak, and whirl signs are the most common observations identified [5]. CT may also show signs of intestinal ischemia such as submucosal edema, poor or non-enhancement of intestinal wall, pneumatosis intestinalis or pneumoperitoneum in case of intestinal perforation.
As for treatement, some authors have reported successful colonoscopic reduction of cecal volvulus but given the potential for colonic perforation colonoscopy is not advised and surgery is the rule, it diverge from simple detorsion to right colectomy. If gangrene or perforation are identified, resection is mandatory, and the current method of choice is right colectomy with primary anastomosis or ileostomy depending on perioperative factors [9]. In case of viable intestines surgeons can either perform an isolated detorsion, cecopexy, caecostomy or hemicolectomy. Isolated detorsion is associated with a high risk of recurrence, therefore, it should not be used anymore [10]. Caecostomy is no longer used because of higher rate of complications including caecum gangrene, fistula, and leakage. The caecopexy method is relatively a safe procedure but with higher recurrence rate. Therefore, hemicolectomy is the treatment of choice in both viable and non-viable bowel [3,10].
Conclusion
Cecal volvulus is a rare cause of bowel obstruction with unspecific symptoms. The radiological imaging plays a major role in the diagnosis. Clinician’s awareness of this disease should be promoted to avoid any diagnosis’s delay in order to reduce the morbimortality rates.
Declarations
The authors do not declare any conflict of interest.
Ethics approval and consent to participate
Not applicable.
Consent for Publication
Written informed consent was obtained from the patients. A copy of the written consent is available for review by the Editorin-Chief of this journal.
Availability of Data and Materials
The data sets are generated on the data system of the CHU Hassan II of Fes, including the biological data and the interventional report.
Competing Interests
The authors declare that they have no competing interests.
Funding
No source of funding was received.
Author’s Contribution
Is the corresponding author, he participated in the organization and writing of the article and studying the cases with OL. Professor supervised working and validated the figures. Professor and chief of department of radiology MB and MM red and allowed the article for publication.
Acknowledgment
All authors read and approved the final manuscript
References
1. Bandurski, R., ZarÄ?ba, K., & KÄ?dra, B. (2011). Cecal volvulus as a rare cause of intestinal obstruction. Polski Przeglad Chirurgiczny, 83(9), 515-517.
2. Khaniya, S., Shakya, V.C., Koirala, R., Pokharel, K., Regmi, R., Adhikary, S., & Agrawal, C.S. (2010). Caecal volvulus: a twisted tale. Tropical doctor, 40(4), 244-246.
3. Berger, J.A., van Leersum, M., & Plaisier, P.W. (2005). Cecal volvulus: Case report and overview of the literature. European Journal of Radiology Extra, 55(3), 101-103.
4. JA, W. (1942). Volvulus of the cecum; Anatomical factors in its etiology: Report of a case. Surg Gynecol Obstet, 74, 882-894.
5. Dane, B., Hindman, N., Johnson, E., & Rosenkrantz, A.B. (2017). Utility of CT findings in the diagnosis of cecal volvulus. American Journal of Roentgenology, 209(4), 762- 766.
6. Tejler, G., & Jiborn, H. (1988). Volvulus of the cecum. Report of 26 cases and review of the literature. Dis. Colon. Rectum. 31, 445-459.
7. Anderson, J.R., Spence, R.A., Wilson, B.G., & Hanna, W.A. (1983). Gangrenous caecal volvulus after colonoscopy. British medical journal (Clinical research ed.), 286(6363), 439–440.
8. Halabi, W.J., Jafari, M.D., Kang, C.Y., Nguyen, V.Q., Carmichael, J.C., Mills, S., ... & Stamos, M.J. (2014). Colonic volvulus in the United States: trends, outcomes, and predictors of mortality. Annals of surgery, 259(2), 293- 301.
9. Katoh, T., Shigemori, T., Fukaya, R., & Suzuki, H. (2009). Cecal volvulus: report of a case and review of Japanese literature. World journal of gastroenterology: WJG, 15(20), 2547.
10. Madiba, T.E., Thomson, S.R., & Church, J.M. (2002). The management of cecal volvulus. Diseases of the colon & rectum, 45, 264-267.
Copyright: © 2025 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.