
Journal of Clinical Review & Case Reports(JCRC)
ISSN: 2573-9565 | DOI: 10.33140/JCRC
Impact Factor: 1.823



Case Report - (2023) Volume 8, Issue 2
An Unusual Presentation of Abrikossoffs Tumor: A Case Report
Received Date: Jan 30, 2023 / Accepted Date: Feb 06, 2023 / Published Date: Feb 15, 2023
Abstract
Granular cell tumors is a rare benign tumor. The malignant GCT (mGCT) form is an extremely rare entity, it can occur in different part of the body, but the spine is a uncommon site. The treatment of choice of Abrikossoff’s tumor is local surgical excision with a wide margin, but in some cases a safe margins cannot be achieved and an adjuvant treatment should be considered.
We report a case of GCT located on the sacral canal with intramedullary extension.
Introduction
Granular cell tumors is a rare benign tumor described for the first time by Abrikossoff in 1926 in a patient with a tongue tumor [1]. Today it is considered that this tumor is probably derived from Schwann cells [2]. It occur mostly in adults between fourth and sixth decade, rarely in children [3]. The most common sites are the head and neck regions (45-65%) [4], it also can be found in skin, gastrointestinal tract, respiratory tract, nervous system, male and female reproductive system [5].
The malignant GCT (mGCT) form is an extremely rare entity, representing approximately 2% of all GCT, and it presentation on the spine is exceptionally rare localization.
We present a case of GCT located on the sacral canal with intramedullary extension.
Case Report
A 42 yeas old women was referred to a neurology department after presenting a back pain evolving for more than two years and lately worsened with movement of legs. The preoperative lumbar magnetic resonance imaging (MRI) show a intramedullary sacral tumor with a double component which was isointense on T2-weighted images, hyperintense on T1-weighted images, and infiltrating the sacral bone structures, the tumor was suggestive of an ependymoma.
The patient then had decreased superficial sensations along with paraplegia in both the lower limbs. A lumbar CT-Scan was performed showing cauda equina compression located on S2. A biopsy was then performed and the final diagnostic was made on the surgical resection, the Immunohistochemical (IHC) stains were positive for CD68, S100, CD163 and SOX10. There was no reaction with epithelial membrane antigen (EMA), glial fibrillary acidic protein (GFAP) and the Ki67<10% The pathologist concluded, after a review with an expert center in USA to a malign Abrikossoff tumor.
Complete excision of the tumour could not be achieved owing to its location. The patient was then treated by adjuvant radiotherapy on the residual tumor of 50 Gy in conventional fractionation with the aim of shrinking the tumor and obtaining a local control.
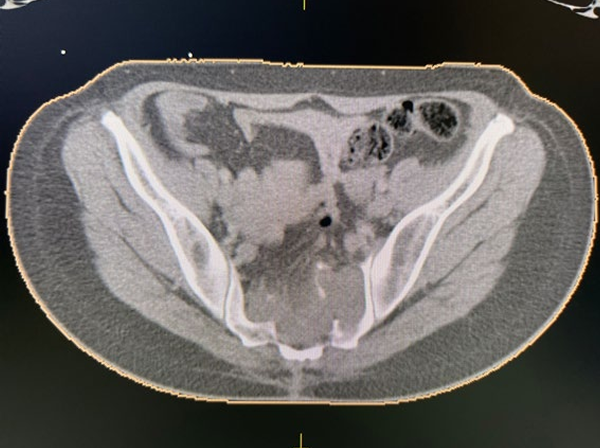
Figure 1: Sacral tumor after resection.
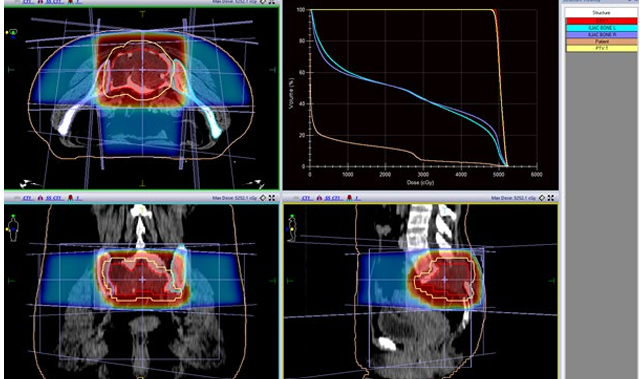
Figure 2: Planning review for 3D radiotherapy: computed tomography scan showing the target volumes: GTV in red, PTV-HR in yellow. (C) delivered dose to the region of high risk, was 50Gy Gy (95% isodose line in red). GTV, gross tumor volume, PTV, planning target volume; HR, high risk.
The follow-up MRI showed a local-regional control. The patient is asymptomatic and her paraplegia was resolved.
Discussion
GCT, also called granular cell myoblastomas is first described by the Russian pathologist Abrikossoff in 1926, involving multiple anatomical sites, but only few cases has been described in spinal cord [6-11].
The histogenesis of Granular cell tumor is unknown. Tumors are believed to be caused by alterations in Schwann cell metabolism. This hypothesis is supported by the persistent presence of the S-100 protein on immunohistochemistry which is also the case for our patient. Clinical symptoms are linked to the tumor site. For tumor who are located in the nervous system, the symptomatology appears as radicular pain, or burning pain, loss of sphincter tone (with bowel and bladder dysfunction), paresthesia etc [7-11].
This spinal tumor are best evaluated by MRI. Tumors are typically slightly hypointense on T1-weighted sequences and show uniform contrast enhancement after intravenous injection of gadolinium. They are generally hypointense on T2-weighted sequences. But similar changes are also seen in other spinal tumors, therefore The histopathologist is responsible for the final diagnosis.
Histopathologically, GCTs consist of large round or polygonal cells with small, dense nuclei. The cytoplasm is enriched with abundant eosinophilic granular substance witch are periodic acid-Schiff (PAS)-positive. Other cancer may also have granular cytoplasm but have other histologic and immunohistochemical features that distinguish them from Abrikossoff tumors [12].
Immunohistochemical analysis provided diagnostic confirmation of granular cell tumour by showing an over expression of S-100 protein, CD68, NSE, inhibin-α, and vimentin. The cells fail to react with GFAP, neurofilament protein (NFP), HMB-45, keratin, EMA, CK7, chromogranin, and synaptophysin. CGTs are usually benign neoplasm, but only few cases 1-10% are malignant. Characteristics that stipulate malignant GCT are, tumor size, rapid growth, presence of metastasis, necrosis, and involvement of adjacent tissue.
Surgical excision is the treatment of choice for malignant CGT. The surgery should accomplished a healthy margins with a 2-3 cm safe margins. In case of incomplete excision, the patient should undergo a revision [13-15], but in some cases, due to the localization, this couldn’t be achieved, and an adjuvant treatment should be considered.
Radiotherapy and chemotherapy have historically been used when malignant tumors are present or when tumors with wide margins cannot be completely resected, but their efficacy has not yet been proven. Although rarely reported, in one case radiotherapy was successfully used to stabilize recurrent/residual disease [17].
This is the case for our patient who a complete resection could not be achieved, and an adjuvant radiotherapy was done (Fgure 1 and 2).
Conflict of Interest Statement
The authors declare no conflict of interest.
References
1. Abrikossoff A (1926) Ueber Myome ausgehened von der quergestreiften willkuerlichen Muskulatur. Virchows. Arch A Pathol Anat 260:215-233.
2. Pushpa G, Karve PP, Subashini K, Narasimhan MN, Ahmad PB, et al. (2013) Abrikossoff’s Tumor: An Unusual Presentation. Indian J Dermatol 58:407.
3. Wright:Chapterinbook:WeissSW,GoldblumJR.Granularcell umour In: Enzinger and Weiss’s (2001) soft tissue tumors. 4thed. St Louis, Mo Mosby; 2001.1178-1187. 4. Ugur K, Emine M, Sevgi K, Sezgin Z (2013) Granular cell tumor on perianal region: a case report. Acta Med Iran 51(7):509-511.
5. Barca I, Cordaro R, Giudice A, Cristofaro MG (2020) Abrikossoffʼs tumor of the tongue: report of three cases and review of the literature. J Oral Maxillofac Pathol 24:S101-s105.
6. Abrinkossoff A (1926) Über Myome, Ausgelend von der quergestreiften willkürlichen Muskulatur. Virch Arch A Pathol Anat Histopathol 260:215-233.
7. Takayama Y, Hasuo K, Takahashi N, Nishimiya M, Nonoshita T, et al. (2004) Granular cell tumor presenting as an intradural extramedullary tumor. Clin Imaging 28:271-273.
8. Critchley GR, Wallis NT, Cowie RA (1997) Granular cell tumour of the spinal cord: Case report. Br J Neurosurg 11:452454.
9. Burton BJ, Kumar VG, Bradford R (1997) Granular cell tumour of the spinal cord in patient with Rubenstein-Taybi syndrome: case report. Br J Neurosurg 11:257-259.
10. Qu J, Ma J, Luo L, Ai L, Li S, Dai J (2009) Subdural granular cell tumor in thoracic vertebral canal. Neurol India 57:679680. 1
1. Weinstein BJ, Arora T, Thompson LD (2010) Intradural, extramedullary spinal cord granular cell tumor: A case report and clinicopathologic review of the literature. Neuropathology 30:621-626
12. Ortiz-Hidalgo C, de La Vega G (1997) Granular cell tumor (Abrikossoff tumor) of the clitoris. Int J Dermatol 36(12):935937.
13. Tawfiq N, Sabri S, Saiss K, Bouchbika Z, Benchekroun N. Jouhadi H, et al. (2013) granular cell tumor: report of a complicated vulvar localization of pulmonary metastases. Cancer Radiother J Soc Francaise Radiother Oncol 17(7):671674.
14. Cheewakriangkrai C, Sharma S, Deeb G, Lele S (2005) A rare female genital tract tumor: benign granular cell tumor of vulva: case report and review of the literature. Gynecol Oncol 97(2):656-658.
15. Aksoy S, Abali H, Kilickap S, Harputluoglu H, Erman M 2006) Metastatic granular cell tumor: a case report and review of the literature. Acta Oncol Stockh Swed 45(1):91-94.
16. Rosenthal SA, Livolsi VA, Turrisi AT (1990) Adjuvant radiotherapy for recurrent granular cell tumor. Cancer 65(4):897-900.
17. Burton BJ, Kumar VG, Bradford R (1997) Granular cell tumour of the spinal cord in patient with Rubenstein-Taybi syndrome: case report. Br J Neurosurg 11:257-25
Copyright: © 2025 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.